Introduction to the Bioarchaeology of Care
In early Neolithic Vietnam, a young man survived from early
adolescence into adulthood completely paralysed from the waist down and with
very limited use of his upper body. Dependent on others for meeting his most basic needs, Burial 9’s
survival was only possible because of the high quality, dedicated and time-consuming
care he received.
The skeletal remains of Man Bac Burial 9, shown in Figure 1 below, provide
evidence of a pathological condition difficult to manage successfully in a
modern medical environment. Four
thousand years ago, the challenges to health maintenance and quality of life
would have been overwhelming.
Figure 1: Man Bac Burial 9 in situ.

Looking after those who are unable to look after themselves is a
behaviour that defines what it is to be human. Evidence suggests health-related care has been
practiced within the human family at least the last 100,000 years, and some
biologists claim that conspecific caregiving was essential to human
evolution.
Certainly, our response to the health needs of others embodies a
wealth of information about ourselves and our community, reflecting cultural
norms and values; collective knowledge, skills and experience; social and
economic organisation; and, more prosaically, access to the resources which allow
the support of someone experiencing disability. It follows that where healthcare practice can be identified in the
archaeological record it has the potential to provide important - and possibly
unique - insights into the lives of those under study.
This is where the bioarchaeology of care comes in.
‘Bioarchaeology of care’ can be employed as an umbrella term to
include any and all bioarchaeological research into health-related care provision. More
narrowly defined, it's a term I appropriated in my PhD research to describe
a specific methodology I’ve developed for identifying and interpreting evidence
for health-related care (Tilley 2013).
In what follows I’m going to describe this new approach.
Definitions, qualifications and caveats.
First, some background. In archaeology,
the experience of pathology during life is expressed in human remains through
lesions in bone or anomalies in preserved soft tissue. Health-related care provision is inferred
from physical evidence that an individual survived with, or recovered from, a
disease or injury likely to have resulted in serious disability. ‘Care’ is operationally defined as the
provision of assistance to an individual experiencing pathology who would
otherwise have been unlikely to survive to achieved age-of-death. ‘Disability’ refers to a state (temporary or
longer-term) arising from an impairment in body function or structure that is associated
with activity limitations and/or participation restrictions, and given meaning
in relation to the lifeways in which it is experienced.
What healthcare comprised depended on the nature of disability,
context in which it occurred and care recipient characteristics. For bioarchaeology of care research purposes, this
care may be divided into ‘direct support’ (e.g. provisioning, nursing, physical
therapy) or ‘accommodation’ of difference (e.g. strategies that enable a level
of participation in social and/or economic activity). Care may begin as ‘support’ and convert to ‘accommodation’
as an individual recovers (but is left with some disability) - or vice versa.
There are obvious provisos. Care can only be inferred with reference to
what is known about the contemporary social, cultural, economic and physical
environments. What constitutes health,
disease and disability is understood very differently in different cultures;
the bioarchaeology of care can only postulate disability where there is
evidence of significant physical impairment. Furthermore, everybody experiences disease in
their own way - disability for one person may not be a disability (or not the same disability) for another. Assumption of the need for care – as well as the
conclusion that care was provided - must always err on the side of caution.
Finally, the bioarchaeology of care approach can only be employed at
a case-study level - at least when dealing with skeletal remains (the focus of
the rest of this article). Most
pathologies won’t ever manifest in bone, and this means that in any prehistoric
community the extent of past burden of disease - and consequently frequency of
caregiving in response to this - must remain unknown.
Interrogating the evidence
for caregiving: the bioarchaeology of care methodology.
The bioarchaeology of care methodology comprises four distinct
stages of analysis, each building upon the observations and conclusions of the previous
one. Although unplanned, these stages
parallel those of Christopher Hawke’s famous ‘Ladder of Inference’ - the first stage
concentrating on description and measurement, and the last wholly dedicated to
interpretation.
All stages of the bioarchaeology of care necessarily derive from the
set of human remains displaying evidence of disability. These remains possess the dual identity of ‘actor’
and ‘artefact’; actor, because the skeletal elements represent a once-living
person who faced the challenges of disability, and artefact because the
skeletal indicators of disability only exist by virtue of the care that helped
this person to survive long enough for the pathology to register in bone. This reading of the bones as simultaneously
signifying individual (subject), and invention (object), underpins the analysis
of care in prehistory.
Stage 1 is triggered by human remains showing evidence of living with, or following,
a serious pathology. It records every
aspect of the remains, their recovery context, and details of contemporary lifeways.
Indicators of pathology are described,
and diagnosis is attempted. If specific diagnosis
is impossible, lesion characteristics may still provide clues to disease impact.
The information recorded at Step 1 is
the foundation for all subsequent analyses.
Stage 2 considers the likely clinical and functional impacts of the
pathology on the subject.
Modern clinical sources are used to assess likely clinical impacts. Human biology has remained the same over
millennia, allowing extrapolation from current knowledge of disease symptoms
and complications. Tuberculosis or a compound
limb fracture elicited the same basic physiological responses in the past as they
do in the present.
Estimating functional impact looks at the likely demands, obstacles
and opportunities in the contemporary lifeways environment, and evaluates the probable
effects of pathology symptoms on the subject's ability to undertake tasks of daily
living, or to participate in their community, without assistance.
The goal of the second stage is to establish whether, on balance of
probability, the individual experienced a disability requiring either ‘direct
support’ or ‘accommodation’ in order to survive. If the answer is yes, then we infer care.
Stage 3 identifies what - in broad terms - this care likely comprised. The goal is to produce a ‘model of care’
within the parameters of the possible and the probable given the contemporary
context. This model also considers how
many people may have been involved in caregiving (in small groups care likely
involved most members, to compensate for increased resource demands and/or
reduced economic contribution of caregivers) and duration of care-provision.
The fine details of care will always be inaccessible. For example, in any particular case we can't
know whether herbal remedies were used, or whether caregiving required prayers,
spells, or exorcism. But basic practices
don’t change. Haemorrhages must be
staunched; bedridden individuals kept well-nourished, clean, comfortable, and
regularly repositioned to aid circulation and prevent pressure sores; people
with high fever kept hydrated. Often the
more practical components of treatment can be deduced with some confidence from
knowledge of the likely clinical and functional impacts of disease.
Stage 4 unpacks and interprets the model of care developed over the first
three stages. It explores what the constituent
elements - singly or in combination - suggest both about contemporary social
practice and social relations and about group and individual (care-recipient) identity.
While each case of care is unique, there is a fundamental principle to
be observed in all cases of health-related
care: recognition that care is the product of agency. Caregiving is an intentional, goal-directed response
to a perceived health crisis, and often consists of complex, inter-related, continuously-refined
and negotiated behaviours carried out over time. The decisions reached in relation to giving and receiving care hold the key to
interpretation, and Stage 4 focuses on the likely choices made (and aspects of
identity underlying these) that contributed to achieving the care outcomes observed
in the skeletal remains under study.
In relation to caregiving,
questions might consider, for example, what options were likely available for
caring, which appear to have been adopted, and why; comparison of the potential
costs and benefits of choices available and those selected; what the ability to
provide care suggests about group organisation, practice and history; and what
the decision to give care, as well as the type and extent of care given,
suggest about general norms and values of the group.
In relation to receipt of
care, a picture is drawn of what, within that lifeways context, the likely ‘normal’
role of someone from the same demographic as the care-recipient may have
been. What was the likely impact of
disability on the care-recipient’s ability to fulfil this role? What alternative roles were available? What sort of personality characteristics
might have been needed to manage pathology-imposed limitations - and what sort
of personality might have inspired others to support or accommodate this
particular individual’s needs, possibly in difficult circumstances? Attempting to identify characteristics of a
person known only through their bones is speculation, but it’s speculation
based on a solid platform of reasoning. There
is little as intimate as the experience of disability. We can never know with certainty how a
prehistoric individual coped, but in cases of extreme disability we might be
able to infer some broad character traits and behavioural strategies that were
called upon.
Figure 2 illustrates the bioarchaeology
of care methodology in action, using the example of the young man from
Neolithic Vietnam introduced earlier. Although
abbreviated, it gives some idea of the information available from the remains
of someone who lived with disability (see Tilley and Oxenham [2011] for detail).
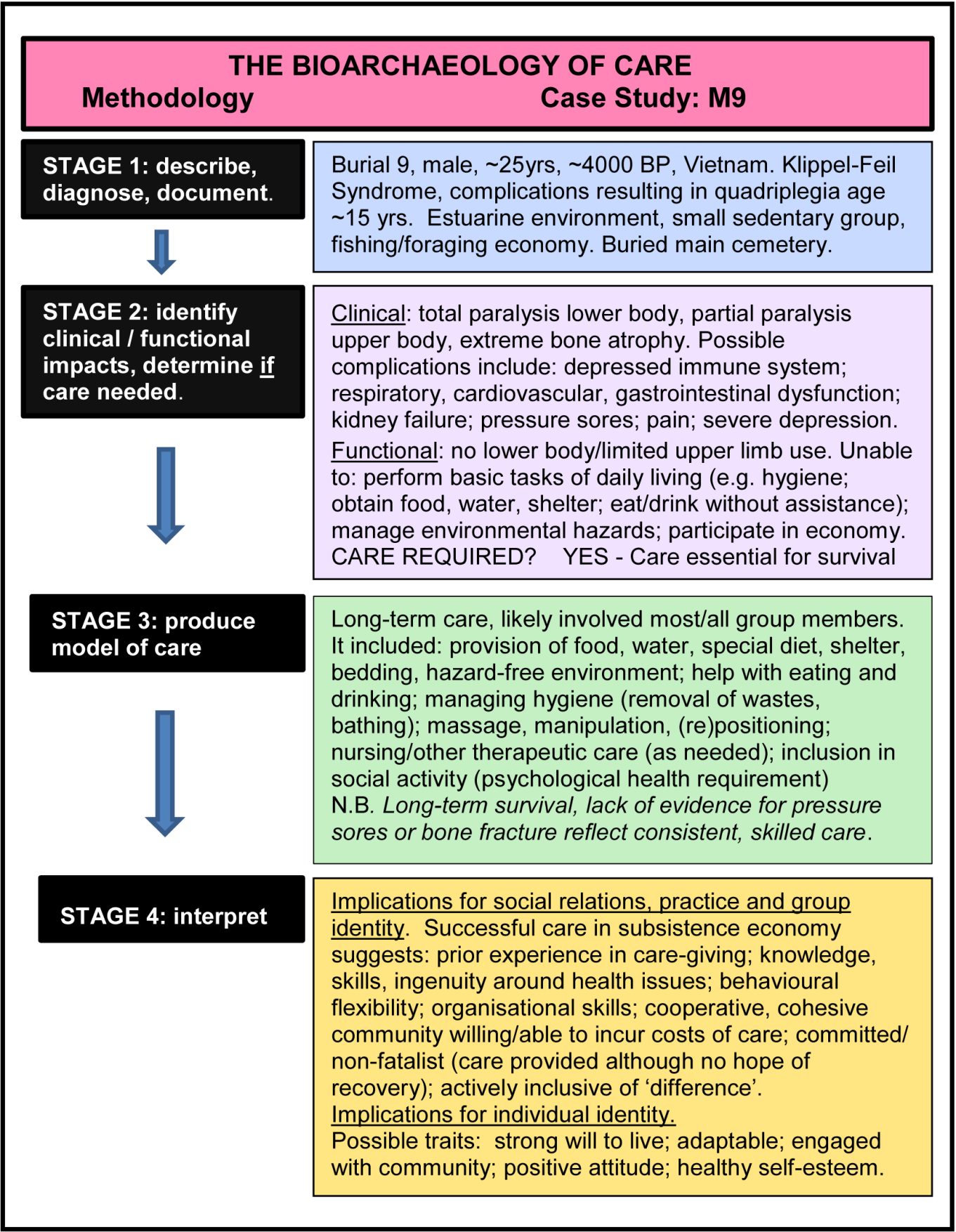
Figure 2: The four stages
of the bioarchaeology of care methodology applied to the case of Man Bac Burial
9.
What next - and why?
In the bioarchaeological literature there are many cases of survival
with disability. For example, the
Neandertal Shanidar 1 survived cranial trauma, amputation of the right arm, various
other injuries, and osteomyelitis (Solecki 1971; Trinkaus and Zimmerman 1982) - suggesting ‘support’ during acute
injury and ‘accommodation’ afterwards. Born
with a mesomelic form of dwarfism, Romito 2 survived in mountainous, Mesolithic
Calabria (Frayer et al. 1987); his remains display upper and lower limb abnormalities
rendering ‘normal’ male hunter-gatherer activity impossible - suggesting
‘accommodation’. In the early Italian
Neolithic a woman survived for years with the increasingly savage effects of
tuberculosis (Canci et al. 1996), impacts of which include pulmonary haemorrhage,
respiratory infection, fever, pain and finally, in this instance, spinal
disintegration resulting in reduction or loss of lower body mobility - suggesting
initial ‘accommodation’ followed by ‘support’.
In some studies the likelihood of care is acknowledged,
although not elaborated. But in most it’s
ignored, and valuable information is lost. Wherever evidence in human remains meets the
criteria for inferring care, there is a role for a bioarchaeology of care
analysis.
Our knowledge of what happened in prehistory will always be partial. When we focus on issues such as care, that
are intrinsically emotive, value-laden, and ultimately reliant on
interpretation, it will also be contentious. However, the bioarchaeology of care methodology
provides a structured, systematic and transparent framework for analysis, enabling
inference and interpretation to be scrutinised, challenged and - where
appropriate - changed.
Equally importantly, a bioarchaeology of care focus opens the way to
a level of engagement with prehistory that helps us to meet our
responsibilities, as archaeologists, to (re)produce the past in a way that captures
the complexity, the sophistication and the humanity of those who have gone
before. In this case, the focus on caregiving
in the past also provides a new perspective for looking at the meaning and
practice of this behaviour in the present.
Lorna Tilley
Australian National University
lorna.tilley@anu.edu.au